Home birth in the United States is very different from home birth in other developed countries.
Different Midwives
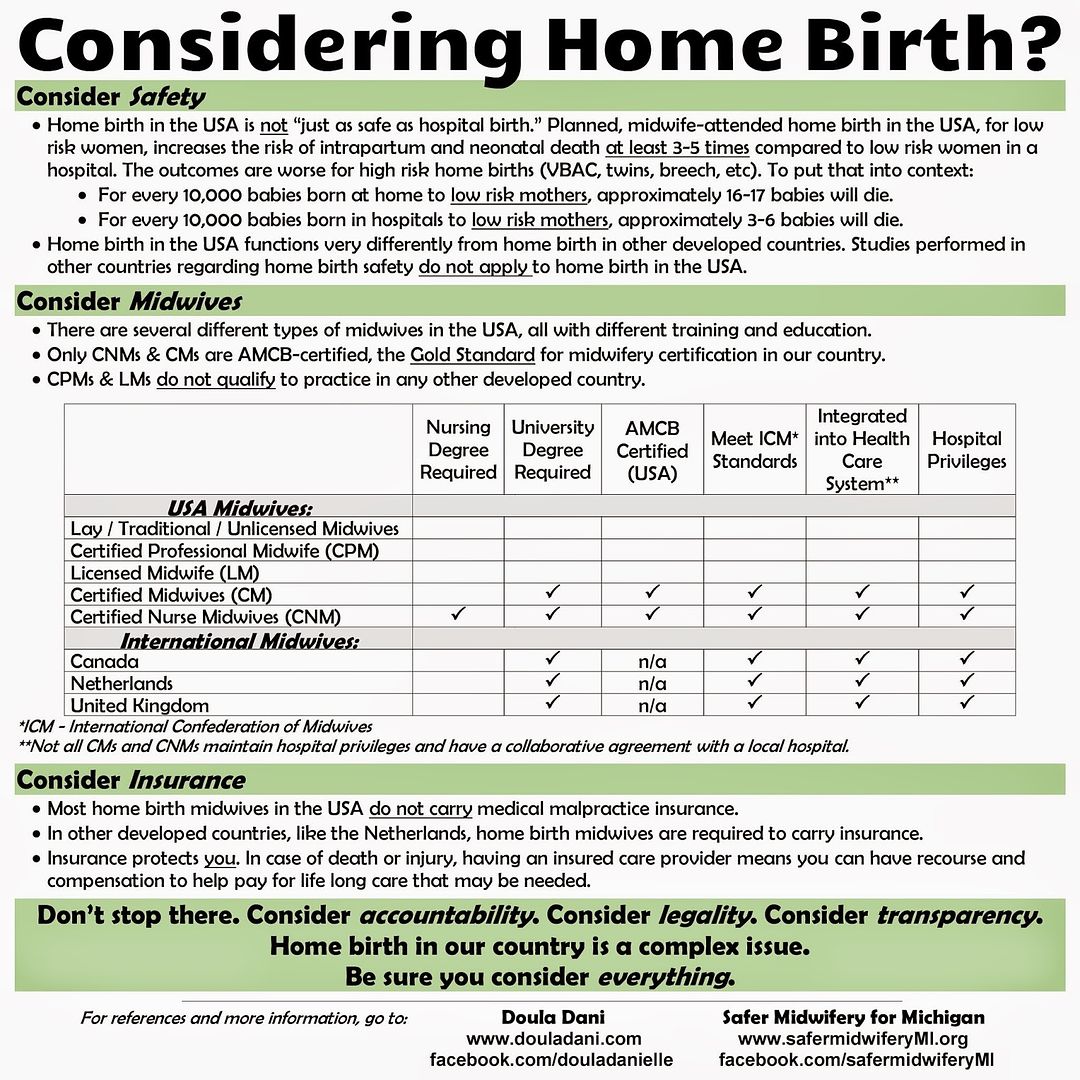
In countries like Canada, the UK, and the Netherlands, the midwives have much higher educational standards than US homebirth midwives. They must have a university degree, they meet the standards set forth by the International Confederation of Midwives, they are integrated into the health care system, and they have hospital privileges.
Most home births in the United States are attended by Certified Professional Midwives (CPMs) or Licensed Midwives (LMs). Neither CPMs nor LMs would be able to practice in
any other developed country; their educational standards are just too low. They do not have to have a university degree (if a midwife became a CPM before 2012, she doesn't even need to have a high school degree), their credential does not meet the standards set forth by the International Confederation of Midwives, they are not integrated into the health care system, and they do not have hospital privileges.
Certified Nurse Midwives (CNMs), which do attend some home births in the United States, are much more similar to midwives found in other developed countries. Like the midwives found in the UK, Canada, and the Netherlands, they must have a university degree, they meet the standards set forth by
the International Confederation of Midwives, they are integrated into
the health care system, and they are (usually) able to obtain hospital privileges.
This helpful chart from "
American Home Birth" illustrates the differences between the types of midwives:
Different Systems
In addition to the differences between American midwives and the midwives found in Canada, the UK, and the Netherlands, the home birth systems are completely different.
In Canada, the UK, the Netherlands, and other developed countries home birth is integrated into the main medical system. Midwives are highly regulated and have accountability for their actions and outcomes.
If a woman wants to have home birth, she is assessed by a care provider to make sure that she is "low risk." "Low risk" means she does not have risk factors such as a previous cesarean, twin (or other multiple) pregnancy, breech baby, previous postpartum hemorrhage, and much, much more. These things are not just "variations of normal" - they are complications that increase the risk to woman and baby during pregnancy and labor. The risking out criteria is quite extensive, to make sure that only the lowest-risk women are attempting home birth.
If a woman develops risk factors any time during her pregnancy or labor, her care is transferred to an OB and she delivers in the hospital. The transfer rate is quite high - about 40% in the Netherlands. A high transfer rate is the sign of a
good home birth system - it means the midwives are recognizing risk factors and taking them seriously. Transferring is to keep the woman and her baby safe, as they are no longer safe attempting a home birth with their risk factors.
In the US, home birth is not integrated into the main medical system. There are almost two systems - the hospital system, and the home birth system. Home birth midwifery laws are determined on a state level, and there is an
incredible amount of variation between the states. In general, accountability of out-of-hospital midwives is very low.
In the United States there are no national risking out criteria for women attempting home birth, and the states that do have legally required risking out factors have very few of them. Here is a chart that compares the Dutch risking out criteria to Oregon's risking out criteria:
Dutch Homebirth Standards vs. Oregon Homebirth Standards. And most states have even less risking out criteria than Oregon.
In most states where midwives can legally attend out of hospital births, they are free to take on women of any risk, and pride themselves on their low transfer rates - even though a low transfer rate is a sign that a midwife is either missing risk factors or ignoring them.
For all of these reasons - poor education, training, regulation, and accountability of US midwives, and the large differences in the US homebirth system compared to the homebirth systems in other developed countries - one cannot use studies from other countries to prove that home birth in the United States is safe. One must use home birth data from, and only from, the US to determine safety of home birth in the United States.
.