In trying to understand why the risks of home birth are so elevated compared to hospital birth, it's important
to understand the "qualifications" of home birth midwives.
There are several different types of midwives
in the United States and if you're not familiar with all of them their titles
can sound similar and confusing. CNM, CPM, CM, DEM, LM...what's the difference?
As Danielle Repp explains in her series "
American Midwives":
"There are two midwifery
certifying bodies in the USA: American Midwifery Certification Board (AMCB) and
North American Registry of Midwives (NARM). The AMCB is considered the Gold
Standard for midwifery certification and is the certifying body for Certified
Nurse Midwives (CNMs) and Certified Midwives (CMs); NARM is the certifying body
for Certified Professional Midwives (CPMs). Licensed Midwives (LMs) also fall
under NARM as it is the NARM entrance exam they take. Specific requirements for
LMs may vary by state in order to take the exam."
"So in short, midwives
in the USA basically fall into one of these three categories:
1. AMCB certified
2. NARM certified
3. Uncertified"
She continues:
"1. Certified
Nurse Midwife (CNM)"
"Certified Nurse Midwives (CNMs)
are some of the most highly skilled and educated midwives in the world. The
Certified Nurse Midwife is one of the only types of midwives in the world that
requires a nursing degree. The CNM also holds a master’s degree as the minimum
level of educational requirement (some have doctoral degrees). CNMs must
complete their education through an ACME-accredited midwifery program (ACME =
Accreditation Commission for Midwifery Education). Once completed, they can apply to take the AMCB certification
exam."
"Certified Nurse Midwives are
licensed and have prescriptive authority in all 50 states (and other
territories of the USA). The educational and clinical skills training of the
CNM not only includes pregnancy and birth care but also primary care for women
throughout life, reproduction, infertility, newborn care, andent of
sexually transmitted diseases."
"2. Certified
Midwife (CM)"
"The Certified Midwife (CM)
credential has existed since 1994. The CM is the direct-entry version of the
CNM. While CMs do not need to have a nursing degree, they must take all of the
nursing school pre-requisites (such as anatomy, physiology, microbiology, etc)
and must receive a bachelor’s degree and master’s degree. The CM’s educational
and clinical skills training is similar to the CNMs, as it again not only
includes pregnancy and birth care but also primary care for women throughout
life, reproduction, infertility, newborn care, and management of sexually
transmitted diseases."
"3. Certified
Professional Midwife (CPM)"
"The Certified Professional
Midwife credential ... was developed as a direct-entry route to become an
out-of-hospital midwife. CPMs are not authorized to work in a hospital setting."
"Certified Professional Midwives
do not have any degree requirements. The
only educational requirement is to have a high school diploma, which was
not a requirement until September 1, 2012."
"The Portfolio Evaluation Process
(PEP) is a popular route to become a CPM. It is an apprenticeship where the
student midwife follows and learns from a preceptor midwife. After attending 40
births (and the prenatal exams leading up to it), the student midwife can
qualify to take the NARM exam. Anyone with a desire to become a midwife can
seek out a preceptor. Half of CPMs have earned
their credential through the PEP route."
"Another route to become a CPM is
to graduate from a Midwifery Education Accreditation Council (MEAC) school.
There are nine MEAC schools in the USA, some of which award certifications,
some diplomas and some degrees."
"CPMs ...do not have prescriptive authority in any states (in certain states, CPMs are
able to obtain certain medications, such as Pitocin, Cytotec, antibiotics, etc
but CPMs cannot write prescriptions). CPMs also
would not qualify to practice midwifery in other developed countries
due to the lack of formal education requirements; the CPM requirements also
do
not meet the International Confederation of Midwives (ICM) standards."
The above was all from Danielle
Repp's series American Midwives,
part 1,
part 2, and
part 3; emphasis mine.
Due to the variation in types of training accepted to become a CPM, some CPMs might have enough education to meet the ICM minimum standards. However, the CPM credential itself does not require it, and
ACOG estimates that "possibly as many as two-thirds of CPMs do not meet the ICM standards."
I want to repeat - Certified
Professional Midwives - the kind of midwives that attend the majority of the home births in the United States -
do not have
any educational requirements other than a high school degree. And if they
became a CPM before 2012, they don't even need that. They don't need to take anatomy, or physiology, or immunology, or even basic college biology.
And do you know what's even worse? In some states, midwives do not have to have
any qualifications at all to practice.
None. The
state where I spent my college years - Utah - has voluntary licensure,
which means that if a midwife simply decides that she'd rather not be
licensed by the state, she has no educational requirements, no limits on
her scope of practice, and no accountability for her actions.
This satirical website points out the weaknesses in such a system.
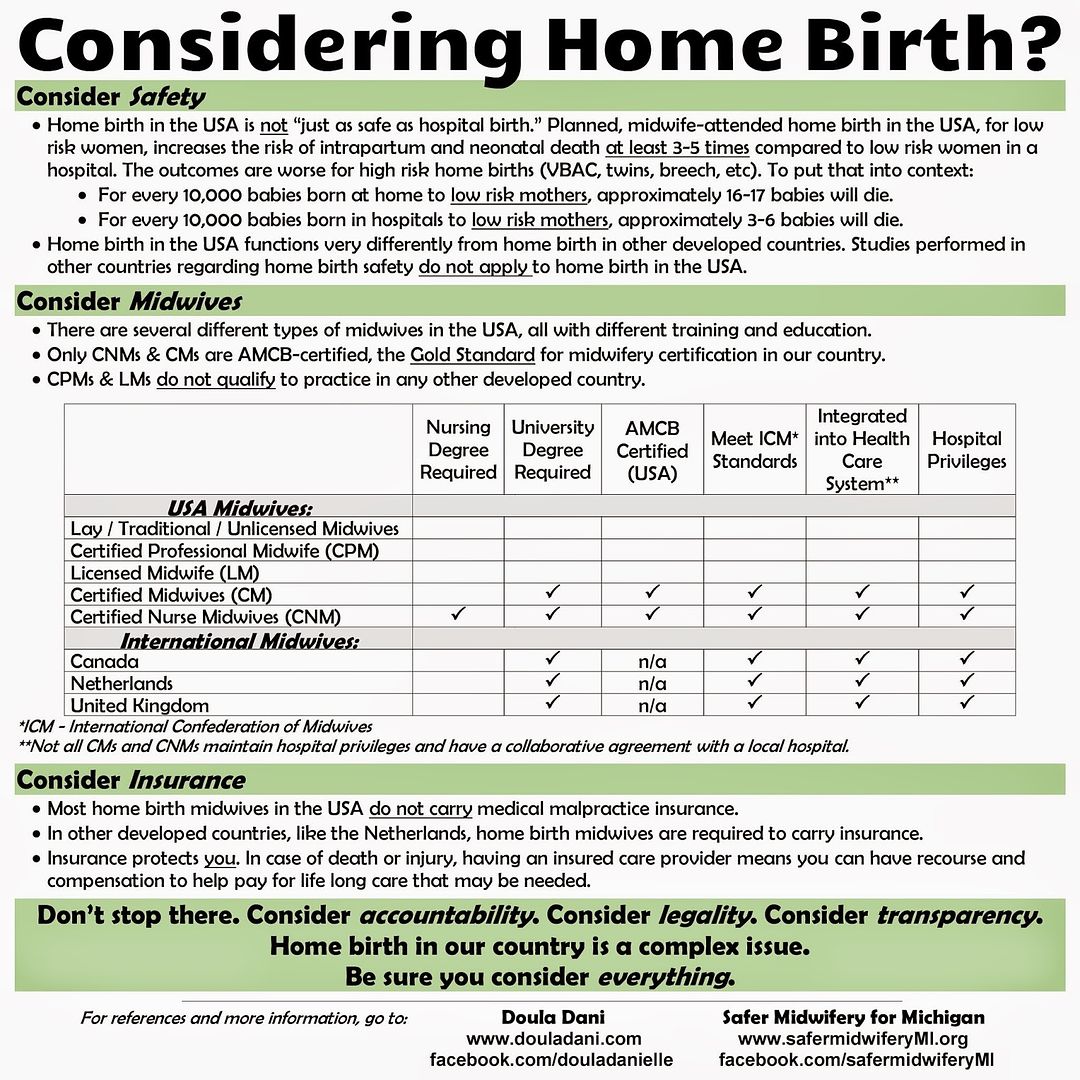
Here are a couple charts that explain the difference between the
midwives who work at doctors offices and in hospitals (CNMs) and the
majority of home birth midwives (CPMs, LMs, lay midwives, etc.):
Now, if you think you'll be safe at home birth if you choose a CNM instead of a CPM, think again.
Researchers in 2009
found that home birth with a CNM had twice as many babies die than
hospital birth with a CNM. An
even more recent study published in 2016 found that babies born to CNMs and CPMs at home birth died three to four times more often than babies born at the hospital, with no statistically significant difference between home births with CNMs or CPMs. Even if your midwife is a CNM instead of a
CPM, you still won't be able to tell at home if your baby is being
deprived of oxygen, you won't have an operating room if it becomes
urgently needed, and you won't have a neonatal resuscitation team with
all of the equipment that might be needed to save your baby.
More excellent articles that explain the disparity between US home birth
midwives and US hospital midwives and the home birth midwives in other
countries can be found here:
The hypothetical situations you can imagine when you think about home
birth midwives' lack of education and regulation - like, "If I have an emergency during labor at home, will my midwife know
what to do? Will she have the skills and training to save my baby?" -
clearly
actually happen at home, as we can see from the numbers.
With home birth midwives, three times as many babies die. With home birth midwives, seventeen times as many babies have brain injuries. These
are the numbers that result from the faulty regulation and extremely low
educational requirements required of US home birth midwives.