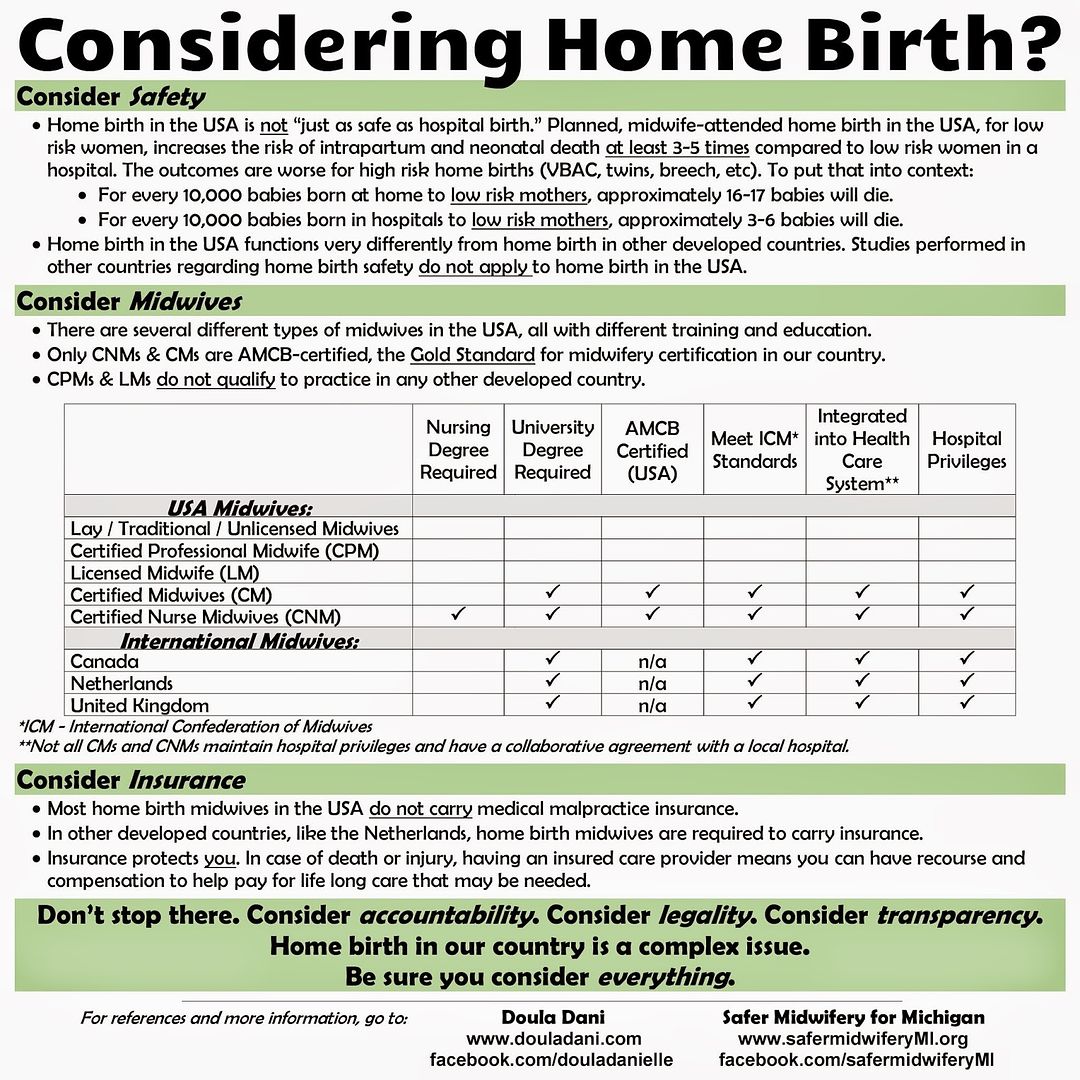
Families thinking about home birth are often told, either by their midwives or by the blogs and websites that advocate for home birth, that "Birth at home is as safe or safer than the hospital." It is not. Every study on American home birth has shown it to have a significantly higher death rate than the hospital.
"But what about the studies on MANA's website?" some ask. That's a good question. On their website, the Midwives Alliance of North America has a section called "Research" in which they have six subsections (A-F) of studies which they say prove the safety of home birth.
Leigh Fransen, former CPM, LM, and part-owner of a birth center and author of the blog Honest Midwife, has gone through and helpfully summarized all of these studies.
After she finally read all of these studies after years of practicing as a midwife, what the data showed shocked her and eventually led her to leave the profession:
"The hours I had spent combing over all of MANA’s best evidence led me
to this conclusion: nonhospital birth might be as safe as hospital
birth, but likely only in health systems in which midwives are
hospital-trained and well-integrated, and where exclusion criteria are
strictly observed to permit only the lowest risk women to proceed.
Nonhospital birth in the United States as currently practiced is
responsible for lower numbers of interventions (such as cesarean section
and medical pain relief) but a substantially higher risk of death or
injury to the baby.
Unbelievably, our 'own' evidence, upon close inspection, was almost unanimously against us."
Unbelievably, our 'own' evidence, upon close inspection, was almost unanimously against us."
You can read Leigh's summaries of all of the studies from the MANA website here:
Doing My Research
Section I: Meta-analyses and Systematic Reviews
Section II: RCTs and Section III: Cohort and Population Based Studies
Section III: Cohort/Population Studies Continued
Section III: Cohort/Population Studies (Re-Continued)
Section IV: International Observational Studies
Section V: Descriptive Studies
The MANA Study
The Other Side
My Days as a Midwife Close
In her post The Best Evidence MANA Does Not Want You To See, she writes:
"In my paper High Risk,
I reviewed all the literature that the Midwives Alliance of North
America (MANA) claims forms the “best evidence” for the safety of home
birth. I found that most of the studies were either not applicable to
the United States, did not address issues of safety, or actually
demonstrated the opposite of what MANA claimed.
If MANA’s cherry-picked data paints a not-so-happy picture, wait until you check out what happens when you look outside of what MANA wants you to see. The literature on nonhospital birth in the United States is downright frightening. Despite what many midwives claim, these studies look at midwife-attended births, not accidental or unattended home births.
If you have had a nonhospital birth like I have, it is natural and normal to feel defensive about the safety of it. After all, to accept that you put your child at a substantial and unnecessary risk doesn’t feel good, even if you know that you made your decision out of love and a genuine desire to make a gentle, safe choice for yourself and your child. Sometimes knowing the truth hurts. I have accepted that my baby was one of the many lucky ones; I invite you to consider joining me in that realization."
If MANA’s cherry-picked data paints a not-so-happy picture, wait until you check out what happens when you look outside of what MANA wants you to see. The literature on nonhospital birth in the United States is downright frightening. Despite what many midwives claim, these studies look at midwife-attended births, not accidental or unattended home births.
If you have had a nonhospital birth like I have, it is natural and normal to feel defensive about the safety of it. After all, to accept that you put your child at a substantial and unnecessary risk doesn’t feel good, even if you know that you made your decision out of love and a genuine desire to make a gentle, safe choice for yourself and your child. Sometimes knowing the truth hurts. I have accepted that my baby was one of the many lucky ones; I invite you to consider joining me in that realization."